
|
|||
|---|---|---|---|
|
|
Auditory biofeedback for upper limb acceleration of runners with cerebral palsy |
|
|
|
*Center for Biomedical Engineering Department of Biomedical Engineering, Faculty of Electrical and Computer Engineering University of Campinas (Brasil) |
Caio Ferraz Cruz caiofcruz@ig.com.br Antônio Augusto Fasolo Quevedo* quevedo@unicamp.br |
|
|
|
|
|||
|
|
http://www.efdeportes.com/ Revista Digital - Buenos Aires - Año 10 - N° 92 - Enero de 2006 |
|
|
1 / 1
Rehabilitation through physical activity that took place after World Wars (DePauw & Gavron, 1995) was improved by research in engineering and biomechanics, through development of equipments increasily adequate to sport practice. While the technological focus in adapted sports for individuals with disabilities has been laid mainly on equipments and materials that allow directly the possibility of sport practice, like protheses and ortheses, little emphasis is given to the development of new technological resources that, indirectly, could improve the athletic performance while contributing to motor learning, usually a n issue for individuals with disabilities (Cidade, Tavares, & Ladewig, 1998).
A valuable tool in motor learning and relearning of individuals with disabilities is biofeedback, that refers to the process of monitoring physiologic events in humans, generally through electronic devices, and displaying information in form of visual or auditory signals, in such a way that the user can learn to self-regulate the physiologic function formerly involuntary (Basmajian, 1989; Bilodeau as cited in Wolf, 1985; Okamoto, 1990). Biofeedback works evoking exteroceptive systems that can replace inadequate proprioceptive signals, allowing the central nervous system to reestablish appropriate sensory-motor nets under voluntary control (Wolf & Binder-Macleod, 1989).
Accelerometers are devices that have received little attention, but that can have, according to Wolf (1985), excellent potential to provide feedback during athletic competitions, improving movement fluidity. Changes in speed when a limb segment move from a point to another are represented as voltage output in the accelerometer.
Wolf and Binder-Macleod (1989) report that auditory feedback over motor activity must be important and maybe easier to process than visual feedback signals. Patients in training of electromyographic feedback frequently will leave the visual signal to look at their limbs while listening to the auditory signals.
According to the model of perceptive-motor cycle of Bueno and Resa (1995), individuals with CP may have problems in input, output, and feedback stages. For those people, biofeedback has been used with success in motor rehabilitation (Colborne, Wright, & Naumann, 1994; De Bacher, 1989; Toner, Cook, & Elder, 1998). Most individuals with CP (70%) are the spastic type, which is characterized by increased reflexes and tonus (Sherrill, Mushett, & Jones, 1988), resulting from damage in motor areas of the brain (Porretta, 1995). Rasch and Burke (1977) state that the spasticity occurs for anti-gravitational muscles, that is, upper limb flexors and lower limb extensors. Rothwell (1994) asserts that spastic paralysis does not occur only in anti-gravitational muscles, but it is greater in flexors than extensors for upper limbs, and the opposite happens for lower limbs. The characteristic posture comprises internal rotation of legs and flexion of elbows, wrists, and fingers (Fallon, 1995). Porretta (1995) reports that there are flexion and internal rotation of hips, flexion of knees, and plantar flexion, which causes the known "scissors gait". With narrow support base, people with this gait pattern generally have problems in balance and locomotion activity.
The posture of individuals with CP causes many disadvantages during running: shorter stride length, less horizontal velocity, greater support time to nonsupport time ratio, smaller hip range of motion (Davids, Bagley, & Bryan, 1998; Pope, Sherrill, Wilkerson, & Pyfer, 1993), and smaller shoulder range of motion (Pope et al., 1993).
The role of upper limbs in running is not negligible. Movements of shoulder and elbow joints are important during running in order to balance the body (Hubbard as cited in Pope et al., 1993; James & Brubaker as cited in Pope et al., 1993; Tetreault & Tetreault, 1988), avoid the undesirable rotation of trunk (Atwater as cited in Pope et al., 1993; Cooper & Glassow as cited in Pope et al., 1993; Jacoby, 1983), help to raise and lower the center of gravity (Cooper & Gassow as cited in Pope et al., 1993; Dyson as cited in Pope et al., 1993), provide a great amount of impulsion (force transference) (Jacoby, 1983), and lower the impact of foot contact (Dyson as cited in Pope et al., 1993).
Tetreault and Tetreault (1988) report that, for long distance runners, upper limbs are important to keep the balance and should be kept low, near the waist line and so relaxed as possible. For sprint runners, upper limbs should swing in a vigorous alternated movement from shoulders and be kept a little higher than waist line.
The angle between arm and forearm, that is, the elbow joint, is kept at about 90º (Fernandes, 1979; Hay, 1981). Arms swing to back and forward from shoulders (Fernandes, 1979; Hay, 1981; Tetreault & Tetreault, 1988). In the forward limit of swing, the hands are about the shoulder height and in the back limit of swing they are at hip level or slightly back (Hay, 1981). Considering that the trunk angle to the horizontal plane is 80-84º (Pope et al., 1993) and the ratio between the forearm and arm lengths is 0.90, according to Rasch (1991), and 0.91, according to Hall (2000), by trigonometry we can conclude that the shoulder joint range of motion is about 100º.
For sprint runners with CP, Pope et al. (1993) verified that the mean shoulder range of motion during running varied from 66º to 85º, that is, less than the shoulder range of motion of runners without disabilities. They have also verified that there was greater range of motion in the shoulder of non-affected or less affected side of hemiparetic runners.
In the elbow joint, the mean range of motion for sprint runners with CP varied from 43º to 77º (Pope et al., 1993), greater than the range of motion reported by Hinrichs (1985) for runners without disabilities, which was 40º.
Having in mind that upper limbs play an important role in running, the objectives of this research were: (1) to test a portable binary auditory biofeedback device for runners with spastic CP to increase, during running, the acceleration of affected upper limb; (2) to verify whether the frequent use of the biofeedback device decreases the need of movement correction; and (3) to verify whether the new movement pattern increases the running velocity.
MethodParticipants
Two male athletes of CPSP (Paraplegics' Club of São Paulo) voluntarily participated in the experiment. They were skilled runners with spastic hemiparetic CP, class 7 of CP-ISRA (Cerebral Palsy International Sport and Recreation Association), and were not taking any medicine for spasticity control.
Following, we describe individual characteristics of the participants:
Athlete 1: 27 years-old, left side affected, previously submitted to tenotomy for lengthening of left plantar and calcanear tendons, experience of two years running, specialist in half distance and long distance.
Athlete 2: 25 years-old, right side affected, experience of two and a half years running, specialist in sprint, first place in Brazilian Championship (100 m, 200 m, and 400 m).
The sample is small because of the lack of Brazilian athletes with CP that regularly train and compete. If, by one side, that reduced sample makes a statistic analysis impracticable, by the other side, it agrees with what Sandweiss (1985) consider the best approach to understand the effects of training on clinical research, that is, to study individual cases and complete descriptive reports.
ApparatusWe developed a portable auditory biofeedback device in the Sensory-Motor Rehabilitation Laboratory of the Department of
Biomedical Engineering at University of Campinas. The device comprises three units:
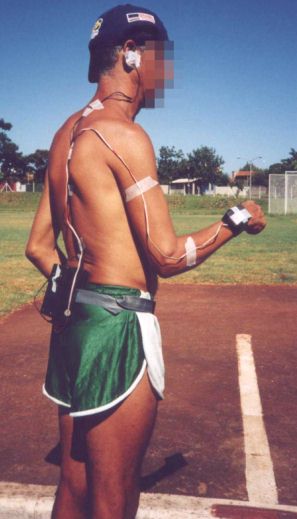
Main unit: a box measuring 8.4 x 12.2 x 6.0 cm, with an electronic circuit that receives the signal from the secondary unit, compares that signal with the pre-set threshold, fires the buzzer if the signal is below the threshold, and counts the number of firings. The main unit has a power switch, a reset switch, an adjustable threshold dial, a line with eight LEDs for binary display of the counter, 9 V battery supply, and an adjustable strip to fix the unit to the athlete's waist.
Secondary unit: a box measuring 4.1 x 5.1 x 2.8 cm that contains an electronic circuit with an ADXL05 accelerometer (Analog Devices, Norwood, USA) to detect the upper limb acceleration at the waist, a flexible cable with a connecting plug to the main unit, and an adjustable strip to fix the unit to the athlete's wrist.
Earphone of 1.6 cm diameter with a flexible cable and a connecting plug to the main unit.
ProcedureBefore the experiment, the participants signed an informed consent form. In a 400 m track at the Olympic Center for Training and Research (São Paulo, Brazil), the athletes have undergone two trials a week. For data acquisition, we fixed the main unit to the athlete's waist, the secondary unit to the athlete's wrist of the affected side, and the earphone to the athlete's ear (Figure 1).
Figure 1. Lateral view of an athlete with the equipment.
Participants received instructions to try to increase the swing speed of the affected upper limb while running each time they heard the auditory biofeedback signal. Before each trial, they warmed up wearing the device, to pre-program their motor reactions and to verify if the device was working correctly.
After warmup, the athletes achieved a trial with their maximum possible speed, each one on the distance he was training that season: 800 m for the Athlete 1 and 400 m for the Athlete 2. A chronometer recorded the time and the device's LED line recorded the number of biofeedback trigger events.
In total, Athlete 1 achieved 38 trials and Athlete 2 achieved 30 trials. In order to verify the track time variation without the device interference, they accomplished maximum effort trials without the equipment: four trials for the Athlete 1 (Trials 1, 16, 31, and 38) and three trials for the Athlete 2 (Trials 1, 16, and 29), besides two races for the Athlete 2 (Trials 17 and 30).
ResultsThe acquired data (track time and number of trigger events) are in Table 1 and plotted in one graphic for each athlete (Figures 2 and 3). The red lines indicate track time variations and the blue lines indicate variations in number of trigger events, along the experiment period. To verify if both variables have decreased along the total period, we have calculated tendency functions, which presented similar behaviors for both cases: linear for track time and second order polynomial for trigger number. The big red squares indicate the maximum effort trials achieved without equipment and the red circles indicate races.
Table 1: Distance Time and Biofeedback Firing Number of Each Athlete

Figure 2 Athlete 1: time and firing number on 800 m
Red continuous line: time; blue continuous line: firing number; red dotted line: time tendency (y = -0.5835x + 200.72);
blue dotted line: firing number tendency (y = -0.0346X2 + 1.5295x - 3.0452); big red squares: maximum effort trials without equipment.Figure 3. Athlete 2: time and firing number on 400 m
Red continuous line: time; blue continuous line: firing number; red dotted line: time tendency (y = -0.2917x + 73.221);
blue dotted line: firing number tendency (y = -0.0297X2 + 0.9751x - 3.5239); big red squares: maximum effort trials without equipment; red circles: races.

Discussion
Athlete 1
The trigger tendency line, given by the second order polynomial y = -0.0346X2 + 1.5295x - 3.0452, shows a parabolic increase until Trial 22 and a latter decrease in number of trigger events.
Regarding the time for 800 m track, although there was great oscillation during the experiment, there was a linear decreasing tendency (about 10% at the end of the period, from about 200 s to about 180 s), according to tendency line given by the equation y = -0.5835x + 200.72. The greatest value was 218 s, recorded on Trial 3, and the smallest value was 175 s, recorded on two trials (25 and 38). There was also a progressive decrease in times of maximum effort trials achieved without the device (Trial 1: 194 s, Trial 16: 184 s, Trial 31: 178 s, and Trial 38: 175 s), all of them below the tendency line.
From the tendency lines for both variables (time and firing), we conclude that the Athlete 1, after 22 trials (parabola peak) increasing the need of biofeedback, learned to run with more swing acceleration of the affected upper limb, decreasing the need of biofeedback. Although his track time decreased, that was not due to his new movement pattern, because this time was already falling while there was increase in trigger number.
Athlete 2
The firing tendency line, given by the second grade polynom y = -0.0297X2 + 0.9751x - 3.5239, shows a parabolic increase until the Trial 16 and a latter decrease in the firing number tendency. However, trying to draw a tendency line of a graphic with such a great variation of values and where the null value appears on most of trials achieved with the device (14 of 25 trials) seems to be a little insensate. We can state that the Athlete 2 already had a movement pattern that allowed him an upper limb acceleration enough for the threshold established in this research and he had a great performance running that way, since he won the first place in the Brazilian Championship, not only on 400 m, but also on 100 m and 200 m.
Regarding the time for 400 m, although there was a great oscillation during the experiment, there was a decreasing linear tendency for track time (fall of about 12%, from about 73 s to about 64 s), according to the tendency line given by the equation y = -0 .2917x + 73.221. The greatest value was 82 s, recorded on the Trials 14 and 18, and the smallest value was 60 s, recorded on two trials (17 and 30), which were races without the biofeedback devide. We must point out that the Athlete 2 won those two races.
There was also a progressive decrease in times of maximum effort trials achieved without the device (Trial 1: 65 s, Trial 16: 64 s, and Trial 29: 62 s), all of them below the tendency line.
We conclude that the Athlete 2 presented little need of correction and no firing in most of trials along the experiment. Therefore, he did not change his movement pattern with the use of the biofeedback device. The tendency of time decrease has no relation with the firing number and must be consequence of another factor of sport training.
Last considerations
Regarding the purposes of this research, we conclude that:
-
The tested biofeedback device was useful to increase the affected upper limb acceleration of runners with CP. Although the Athlete 2 presented little biofeedback need because of his movement pattern, we realized that, when necessary, the feedback was useful. Besides that, the device can be easily handled by the researcher. If there was a display for decimal counting of trigger events, it would be even easier for coaches and athletes to use it. A negative point is the inconvenience reported by the participants: wires strapped on skin and a shaking box in the lumbar region, problems that can be solved in future research with telemetry and miniature devices.
-
The frequent use of the biofeedback device can help decreasing the need of movement correction, that is, the athlete can acquire a new movement pattern, with greater acceleration of the upper limb, if he is not yet in his best performance. From that, we suppose that the device can be pretty useful in motor learning of people with CP that intend to begin a sports program.
-
We could not prove that the new movement pattern (greater acceleration of the affected upper limb), observed just in the Athlete 1, was the cause for increase in running velocity, because the metodology could not separate the effects of the conventional sport training.
More research is necessary, in order to work with a greater sample (more participants and more trials), compare two groups (one with biofeedback and another without it), and separate the effects of the conventional sport training from the biofeedback training.
References
-
Basmajian, J. V. (1989). Introduction: Principles and background. In J. V. Basmajian (Ed.), Biofeedback: Principles and practice for clinicians (3rd ed.). Baltimore: Williams & Wilkins.
-
Bueno, S. T., & Resa, J. A. Z. (1995). Educación física para niños y niñas com necessidades educativas especiales. Málaga: Ediciones Aljibe.
-
Cidade, R. E., Tavares, M. C. G. C. F., & Ladewig, I. (1998). Aprendizagem motora e cognição em portadores de deficiência. Revista da Sociedade Brasileira de Atividade Motora Adaptada, 3(3), 17-20.
-
Colborne, G. R., Wright, F. V., & Naumann, S. (1994). Feedback of triceps surae EMG in gait of children with cerebral palsy: A controlled study. Arch. Phys. Med. Rehabil., 75(1), 40-45.
-
Davids, J. R., Bagley, A. M., & Bryan, M. (1998). Kinematic and kinetic analysis of running in children with cerebral palsy. Developmental Medicine & Child Neurology, 40, 528-535.
-
De Bacher, G. (1989). Biofeedback in spasticity control. In J. V. Basmajian (Ed.), Biofeedback: Principles and practice for clinicians (3rd ed.). Baltimore: Williams & Wilkins.
-
Depauw, K. P., & Gavron, S. J. (1995). Disability and sport. Champaign: Human Kinetics.
-
Fallon, K. E. (1995). The disabled athlete. In J. Bloomfield, P. A. Fricker, & K. D. Fitch (Eds.), Science and medicine in sport (2nd ed.). Carlton: Blackwell Science.
-
Fernandes, J. L. (1979). Atletismo: Corridas (2nd ed.). São Paulo: EPU.
-
Hall, S. (2000). Biomecânica básica (3rd ed.). Rio de Janeiro: Guanabara Koogan.
-
Hay, J. (1981). Biomecânica das técnicas desportivas (2nd ed.). Rio de Janeiro: Interamericana.
-
Hinrichs, R. N. (1985). A three-dimensional analysis of the net moments at he shoulder and elbow joints in running and their relationship to upper extremity EMG activity. In D. A. Winter, R. W. Norman, R. P. Wells, K. C. Hayes, & A. E. Patla (Eds.), Biomechanics IX-B (pp. 337-342). Champaign: Human Kinetics.
-
Jacoby, E. (1983). Applied techniques in track and field. New York: Leisure Press.
-
Okamoto, G. A. (1990). Medicina física e reabilitação. São Paulo: Manole.
-
Pope, C., Sherrill, C., Wilkerson, J., & Pyfer, J. (1993). Biomechanical variables in sprint running of athletes with cerebral palsy. Adapted Physical Activity Quarterly, 10, 226-254.
-
Porretta, D. L. (1995). Cerebral palsy, Traumatic brain injury, Stroke, Amputations, Dwarfism, and other orthopedic impairments. In J. P. Winnick (Ed.), Adapted physical education and sport (2nd ed.). Champaign: Human Kinetics.
-
Rasch, P. J. (1991). Cinesiologia e anatomia aplicada (7th ed.). Rio de Janeiro: Guanabra Koogan.
-
Rasch, P. J., & Burke, R. K. (1977). Cinesiologia e anatomia aplicada: A ciência do movimento humano (5th ed.). Rio de Janeiro: Guanabara Koogan.
-
Rothwell, J. (1994). Control of human voluntary movement (2nd ed.). London: Chapman & Hall.
-
Sandweiss, J. H. (1985). Biofeedback and sport science. In J. H. Sandweiss & S. L. Wolf (Eds.), Biofeedback and sport science. New York: Plenum Press.
-
Sherrill, C., Mushett, C., & Jones, J. A. (1988). Cerebral palsy and the CP athlete. In J. A. Jones (Ed.), Training guide to cerebral palsy sports (3rd ed.). Champaign: Human Kinetics Books.
-
Tetreault, J., & Tetreault, P. (1988). Tracking techniques for track events. In J. A. Jones (Ed.), Training guide to cerebral palsy sports (3rd ed.). Champaign: Human Kinetics Books.
-
Toner, L. V., Cook, K., & Elder, G. C. B. (1998). Improved ankle function in children with cerebral palsy after computer-assisted motor learning. Developmental Medicine & Child Neurology, 40, 829-835.
-
Wolf, S. L. (1985). Biofeedback applications in rehabilitation medicine: Implications for performance in sports. In J. H. Sandweiss & S. L. Wolf (Eds.), Biofeedback and sport science. New York: Plenum Press.
-
Wolf, S. L., & Binder-Macleod, S. A. (1989). Neurophysiological factors in electromyographic feedback for neuromotor disturbances. In J. V. Basmajian (Ed.), Biofeedback: Principles and practice for clinicians (3rd ed.). Baltimore: Williams & Wilkins.
Authors note
-
We thank CAPES (Improvement Coordination of Graduate Staff) for the financial support and the athletes of CPSP (Paraplegics' Club of São Paulo) who have voluntarily cooperated in the experiment.
More articles in English
| |
|
|---|---|
|
revista
digital · Año 10 · N° 92 | Buenos Aires, Enero 2006 |
|